Painful Red Eye — Free SCA Practice Case
Schoolteacher with painful red eye
Station Timer
Golden Minute
Initial Introduction
•Introduce yourself
•Ask an open question — "How can I help you today?"
•Listen — don't interrupt
•Catch early cues
Data Gathering
History, ICE & Diagnosis
Clinical Management
Diagnosis, Plan & Decisions
Safety Net
Follow-up & Close
Materials for Candidate
Please review before starting the consultation
Full Name
Sarah Collins
Age
34 years
Consultation Type
VideoAge
34 (DOB: 14/05/1991)
Reason for Encounter
"My left eye is throbbing and I can barely see out of it. I had to leave school early."
Medical Records
- ●PMH: Generally fit and well. History of lower back pain (under investigation by physio).
- ●Medications: Ibuprofen 400mg PRN.
- ●Allergies: NKDA.
- ●Occupation: Primary School Teacher.
Examination (Visuals provided during consult)
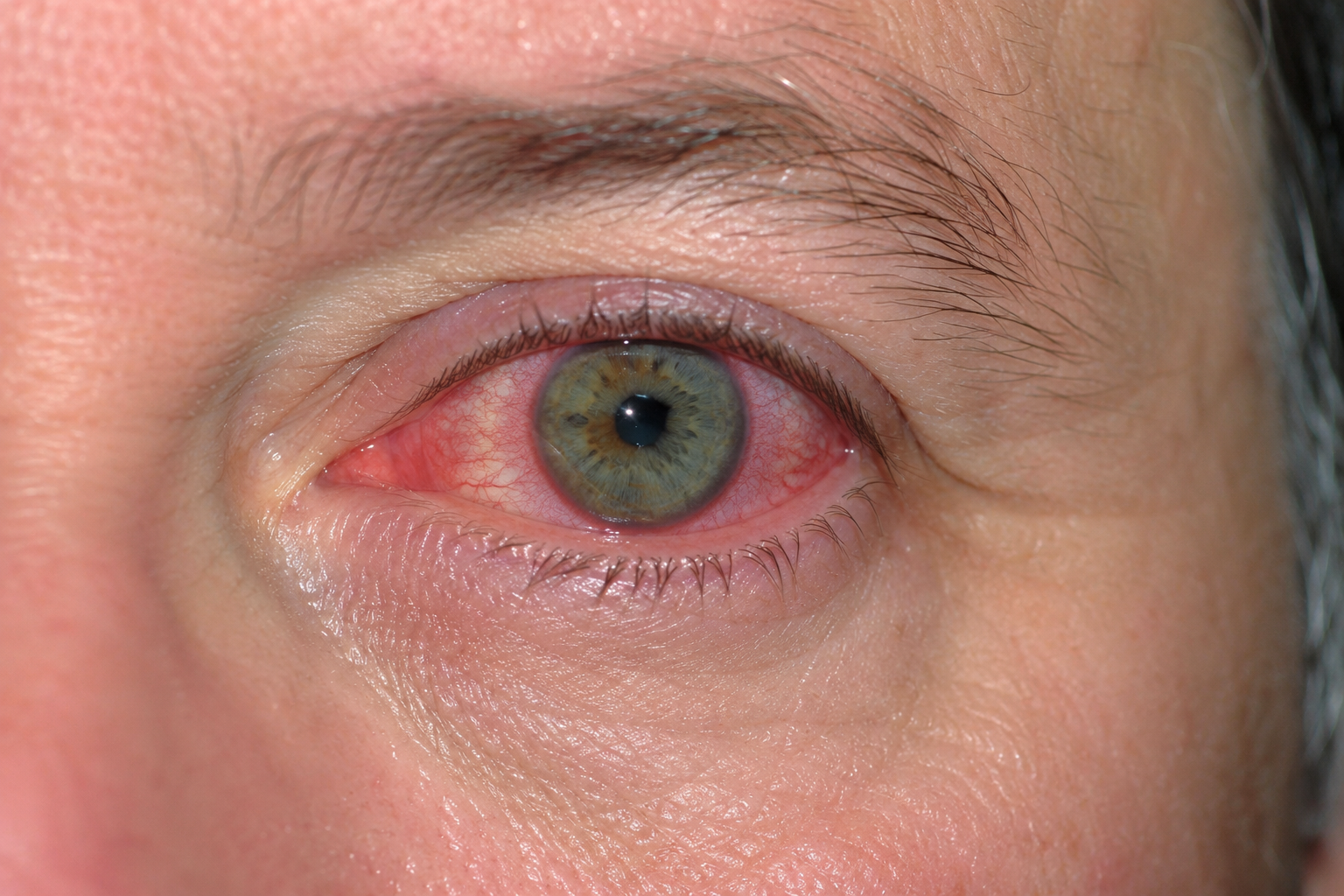
- ●Photograph: The patient uploads/shows a photo of the left eye.
Patient Script
For the friend playing the patient role
Character Overview: You are Sarah. You are usually very stoic, but this pain is grinding you down. You are wearing sunglasses even indoors because the light hurts so much. You are worried you won't be able to mark the children's books or drive.
Opening Sentence: (Wearing sunglasses) "Hi Doctor. I'm sorry about the glasses, but the light is agonizing. My left eye has been aching for two days, but this morning it's blurred and the pain is a deep, dull throb. I can't focus on anything."
History if Asked (Data Gathering Phase)
- ●The Pain: "It's a deep ache, right inside the eyeball. It's about an 8/10. It hurts more when I try to read or look at my phone."
- ●Photophobia (The Key Symptom): "If I take my glasses off or look at a window, I get a sharp stabbing pain. It makes me feel sick."
- ●Visual Changes: "It's like looking through a fog. Everything is blurry."
- ●Red Flag Exclusion:
- ●Discharge: "No, it's not sticky. My eyelids aren't stuck together in the morning." (Rules out Bacterial Conjunctivitis).
- ●Trauma: "No, I haven't been poked or hit."
- ●Contact Lenses: "No, I wear glasses." (Rules out CL-related Keratitis).
- ●Systemic Screen (HLA-B27 Link):
- ●If asked about joints/back: "Funny you ask, my lower back has been really stiff in the mornings recently. It takes me an hour to get moving. I thought it was just from bending over desks." (Clue for Ankylosing Spondylitis).
ICE — Ideas, Concerns, Expectations
(Actor guidance: Do not volunteer any of the following unprompted. Only share these responses if the candidate directly explores your ideas, concerns, or expectations.)
- ●Ideas: "I thought it might be conjunctivitis at first — my class had it going around a few weeks ago. But there's no gunge or stickiness, so I'm not really sure what it is. It just doesn't feel like a surface thing — the pain feels like it's deep inside."
- ●Concerns: "Honestly, I'm scared about my sight. I've never had anything like this before and it's getting worse, not better. I keep thinking — what if this is something serious and I lose the vision in that eye? I'm also panicking about work. Reports are due next week and I can barely look at a screen."
- ●Expectations: "I just want someone to tell me what's actually wrong with it and fix it. I was hoping you could give me some drops or something so I can get back to normal. If it's something more serious, I need to know — I'd rather know than not."
If Asked — Medical History and Medications
(Actor guidance: Respond naturally if the candidate asks about your medical history or current medications. Do not volunteer this information unprompted.)
- ●If asked about current medications: "I take ibuprofen when my back plays up — the 400mg ones. Probably three or four times a week at the moment. I've actually been taking it for the eye pain too, but it's barely touching it."
- ●If asked about allergies: "No, no allergies to anything that I know of."
- ●If asked about the back pain / physiotherapy: "I've been seeing a physio for my lower back. It started about six months ago — this deep stiffness, especially first thing in the morning. The physio said my flexibility isn't great but they're still trying to work out what's going on. I've got some exercises but they don't seem to make much difference."
- ●If asked whether the back pain is worse at rest or with activity: "Definitely worse when I've been still — mornings are the worst. Once I get moving it eases off a bit, but it never completely goes."
Social History and Lifestyle Impact
(Actor guidance: This content can be shared naturally in conversation when discussing how the condition is affecting you. It does not need to be delivered as a monologue.)
- ●Occupation and daily life: Sarah is a Year 2 primary school teacher. Her day involves reading with children, marking books, writing on the whiteboard, and supervising outdoor play — all visually demanding tasks.
- ●Lifestyle impact of the condition: "I had to get my teaching assistant to take over reading groups yesterday because I couldn't see the words on the page properly. I can't mark their books — the handwriting is tiny and I just can't focus on it. I tried to do reports on the computer last night and had to give up after ten minutes because the screen light was agony. I drove to school this morning with one eye shut, which was terrifying. I'm meant to be doing a parents' evening on Thursday and I can't even face the thought of sitting under those fluorescent lights for three hours."
If Asked — Associated Symptoms
(Actor guidance: Only share these responses if the candidate asks about these specific symptoms. Do not volunteer any of this information unprompted.)
- ●If asked about floaters or flashes: "No, I haven't noticed any spots or flashing lights — it's more just that everything is hazy."
- ●If asked about headache: "I've had a bit of a headache on the left side, but I think that's just from screwing my eye up all day. It's not a bad headache on its own."
- ●If asked about nausea or vomiting: "I felt a bit queasy this morning when the pain was really bad, but I haven't actually been sick."
- ●If asked about mouth ulcers: "No, nothing like that." (Pertinent negative — Behçet's disease).
- ●If asked about skin rashes or psoriasis: "No, I've never had any skin problems." (Pertinent negative — psoriatic arthritis / reactive arthritis).
- ●If asked about genital ulcers or urethral symptoms: "No, nothing like that at all." (Pertinent negative — Behçet's disease / reactive arthritis).
- ●If asked about bowel problems (diarrhoea, blood in stool): "No, my stomach is fine." (Pertinent negative — IBD-associated uveitis).
- ●If asked about recent infections (urinary, STI, gastroenteritis): "No, I've been well otherwise — just the back and now this." (Pertinent negative — reactive arthritis).
- ●If asked about fever or feeling generally unwell: "No, I don't feel ill in myself — it's just the eye."
- ●If asked about the other eye: "No, the right eye is completely fine — it's just the left."
- ●If asked about previous episodes of eye problems: "No, I've never had anything like this before. I just wear glasses for reading."
Responses to Management (The Negotiation Phase)
- ●If the Doctor prescribes Antibiotic Drops (Chloramphenicol):
- ●Reaction: "I tried Optrex from the chemist and it stung like crazy. Are you sure it's an infection? There's no pus."
- ●If the Doctor asks to check the eye:
- ●Reaction: "Please be quick with the light, it really hurts." (Wince visibly if they shine a light).
- ●If the Doctor refers to Eye Casualty:
- ●Reaction: "Do I have to go now? I have a class to teach tomorrow. Can't I just have drops?" (Needs explanation of sight-threatening risk).
- ●If the Doctor mentions driving:
- ●Reaction: "I drove here, but I had to keep one eye shut. Is that dangerous?"
Mark Scheme
Domain 1: Data Gathering and Diagnosis
Domain 2: Clinical Management and Medical Complexity
Domain 3: Relating to Others
Clinical Learning Points
Diagnosing Anterior Uveitis: The Key Clinical Features
- ●Anterior uveitis (iritis/iridocyclitis) is inflammation of the iris and ciliary body — the uveal tract anterior to the lens. It is a sight-threatening emergency requiring same-day specialist assessment.
- ●The clinical triad: ciliary flush (circumcorneal redness concentrated at the limbus, fading towards the periphery), miosis (constricted pupil from iris sphincter spasm), and photophobia (pain provoked by light, caused by movement of the inflamed iris).
- ●The pain is characteristically deep and dull — felt inside the eyeball, not on the surface. It worsens with eye movement and accommodation. Surface pain or grittiness suggests conjunctival or corneal pathology, not intraocular inflammation.
- ●Pupil irregularity (non-circular shape) indicates posterior synechiae — adhesions between the iris and the anterior lens capsule. This is a complication that is already developing and reinforces urgency.
Differential Diagnosis: The Three Conditions to Exclude
- ●Acute angle-closure glaucoma: Pupil is mid-dilated, fixed, and oval (not miotic). Vision is severely impaired with haloes around lights. Pain is often accompanied by nausea and vomiting. The eye is rock-hard on palpation. Patient is typically older and hypermetropic. This is an ophthalmological emergency — same-day referral mandatory.
- ●Bacterial conjunctivitis: Mucopurulent discharge with sticky eyelids in the morning. No significant photophobia. Pain is a gritty, surface discomfort — not deep. Vision is normal or only mildly affected by discharge. Pupil is normal. This presentation has none of these features.
- ●Microbial keratitis (corneal ulcer): Associated with contact lens wear (highest risk factor). White opacity or fluorescein-staining ulcer visible on the cornea. Photophobia and pain present but typically more surface-localised. Sarah does not wear contact lenses, making this significantly less likely.
Investigations: Identifying the Underlying Cause
- ●Anterior uveitis does not require investigation in the acute primary care setting — this is the ophthalmologist's role. Do not delay referral to arrange blood tests.
- ●Once the acute episode is managed, investigate for an underlying systemic cause. Relevant investigations include: ESR and CRP (inflammatory markers), HLA-B27 (associated with spondyloarthropathies in approximately 50% of anterior uveitis cases), ANA and rheumatoid factor (to screen for connective tissue disease), and chest X-ray (if sarcoidosis is suspected).
- ●In practice, many of these investigations are initiated by the ophthalmologist or rheumatologist. The GP's role is to coordinate follow-up and ensure the workup is completed — particularly relevant here given Sarah's concurrent inflammatory back pain.
Clinical Management: Acute Episode
- ●Primary care management is referral — not treatment. Do not attempt to treat anterior uveitis in primary care without specialist input.
- ●Same-day referral to ophthalmology (eye casualty) is the correct action. Slit-lamp examination is required to confirm the diagnosis, grade the severity of intraocular inflammation (cell and flare in the anterior chamber), and exclude herpetic keratitis before any treatment is started.
- ●Mydriatics (e.g. cyclopentolate 1%): Pupil-dilating drops prescribed by the specialist. These relieve ciliary spasm (reducing deep pain), prevent posterior synechiae formation, and break down any early synechiae that have already formed. Explaining this to the patient — "the drops will dilate the pupil to stop the pain and prevent the iris sticking to the lens" — helps them understand the urgency of being seen.
- ●Topical steroids (e.g. prednisolone acetate 1%): The mainstay of treatment, initiated by the ophthalmologist. Never start steroid drops in primary care without slit-lamp examination. Herpes simplex keratitis (dendritic ulcer) can mimic anterior uveitis clinically; topical steroids would cause rapid, potentially catastrophic corneal worsening in this setting.
- ●Oral analgesia for the current episode: Advise regular paracetamol and continue ibuprofen if tolerated. Note that this patient is already taking ibuprofen 400mg three to four times per week — counsel on appropriate use, the importance of taking it with food, and consider whether gastric protection (e.g. a PPI) is warranted given her level of NSAID use.
- ●Photophobia relief: Advise wearing sunglasses or remaining in a dimly lit environment until seen by the specialist.
Complications of Untreated or Inadequately Treated Anterior Uveitis
- ●Posterior synechiae: Adhesions between the iris and anterior lens capsule cause permanent pupil irregularity and can progress to pupil block, raising intraocular pressure.
- ●Secondary glaucoma: Raised intraocular pressure from pupil block or trabecular meshwork inflammation can cause irreversible optic nerve damage.
- ●Cataract: Prolonged inflammation and steroid use can both contribute to lens opacification.
- ●Permanent visual loss: The cumulative result of untreated or recurrent inflammation without adequate specialist management.
Systemic Associations
- ●Approximately 50% of cases are idiopathic. The remaining 50% are associated with HLA-B27-related spondyloarthropathies or other systemic inflammatory conditions.
- ●HLA-B27-associated conditions to consider:
- ●Ankylosing spondylitis — inflammatory back pain with morning stiffness lasting over 30 minutes, improving with activity (as in this case). Anterior uveitis is the most common extra-articular manifestation, occurring in up to 40% of patients.
- ●Psoriatic arthritis — ask about skin plaques or nail changes.
- ●Reactive arthritis — follows urogenital or gastrointestinal infection; triad of arthritis, urethritis, and conjunctivitis (Reiter's syndrome).
- ●Inflammatory bowel disease — Crohn's disease and ulcerative colitis; ask about bloody diarrhoea and abdominal pain.
- ●Non-HLA-B27 associations:
- ●Sarcoidosis — bilateral or granulomatous uveitis; associated with bilateral hilar lymphadenopathy, skin, and pulmonary manifestations.
- ●Behçet's disease — rare; triad of recurrent oral ulcers, genital ulcers, and uveitis.
- ●In this case, the inflammatory pattern of back pain (morning stiffness lasting one hour, improving with movement, present for six months) is strongly suggestive of a spondyloarthropathy — most likely ankylosing spondylitis. This connection must be made explicit to the patient and followed up through appropriate rheumatology involvement.
Driving Safety
- ●A patient with monocular blurred vision and severe photophobia is not safe to drive. Photophobia causes dazzle from oncoming lights and sunlight; blurred vision impairs visual acuity in the affected eye.
- ●DVLA guidance states that drivers must meet the required visual standards — monocular vision loss does not automatically disqualify, but active symptomatic disease with visual impairment does.
- ●Advise the patient clearly not to drive until assessed and treated by the ophthalmologist. Arrange or discuss alternative transport to eye casualty. This is a patient safety issue and must not be omitted.
Safety-Netting and Follow-Up
- ●Emergency escalation: If symptoms acutely worsen before the specialist appointment — sudden further loss of vision, severe increase in pain, new floaters or flashes — attend A&E immediately. Floaters and flashes raise concern for posterior segment involvement or retinal detachment.
- ●Recurrence: Anterior uveitis has a significant recurrence rate, particularly in HLA-B27-positive patients and those with an underlying systemic condition. Advise the patient to seek urgent medical attention promptly if she ever experiences similar symptoms in either eye — early treatment reduces the risk of complications.
- ●GP follow-up: The GP's role does not end with the referral. Follow up after the ophthalmology assessment: review the specialist's findings and treatment plan, coordinate investigation of the systemic cause, and liaise with rheumatology regarding the inflammatory back pain workup.
Common Candidate Mistakes in This Case
- ●Diagnosing conjunctivitis and prescribing antibiotic drops (e.g. chloramphenicol): The absence of discharge, the severity of photophobia, and the deep nature of the pain make conjunctivitis untenable. Chloramphenicol treats bacterial surface infection — it has no role here and delays appropriate care.
- ●Prescribing topical steroid drops in primary care: Without slit-lamp examination to exclude herpetic keratitis, prescribing prednisolone or dexamethasone drops is dangerous.
- ●Referring non-urgently or suggesting an optician: Anterior uveitis is sight-threatening. A routine referral or optician suggestion is inadequate — same-day ophthalmology assessment is required.
- ●Treating the eye in isolation: Missing the systemic link to inflammatory back pain is a significant omission in this case. The pattern of inflammatory back pain in a 34-year-old, combined with acute anterior uveitis, should prompt explicit consideration of ankylosing spondylitis and a plan for systemic investigation.
- ●Not addressing driving safety: The patient disclosed she drove to the appointment with one eye closed due to blurred vision. Failing to address this directly is a clinical and safety omission.